

The Foreskin: Why Is It Such A Secret In North America?
The male prepuce, or foreskin, is a highly mobile and extraordinarily sensitive double fold of tissue that is the end of the penis. Why do Americans go out of their way to remove this part of human anatomy, when the rest of the world does not?
Note: Never have I gotten so many comments and emails in response to a blog post, much less rumors that I’m a man. I’ll keep that in mind. And for the record, it wasn’t until 2014 that I had the opportunity to put a man’s intact penis in my very much female vagina. This frictionless appendage made me realize that sex doesn’t have to be painful or cause hazardous inflammation. And with that image in your mind…
I was nineteen or twenty years old when a male friend of mine, we’ll call him Bill, let me in on a most shocking fact: He was missing part of his penis, and so were almost all boys and men that I had ever seen in my entire life, as well as all the anatomical diagrams that I had ever seen. Ever.
Sure, I had heard of circumcision as a Jewish religious practice, but thought myself unlikely to ever see its results. Little did I know, all the male genitalia I had seen both in real life and as depicted in American anatomy books, had been edited in exactly the same way. The shock from this revelation overwhelmed me for weeks, especially since I considered myself to be fairly knowledgeable about anatomy. (My interests included biology and drawing biological structures).
Why would anyone selectively remove foreskins, not just from real people but from scientific anatomical texts, which I had thought were meant to represent the natural human form? And why did no one ever tell me about this? It was as though a basic feature that males (of all mammals) are normally born with was not to be understood or even acknowledged.
I spent the next few weeks at the local library, immersing myself in primary and secondary source materials on the relevant anatomy, medicine and history, before I was satisfied that I had an accurate understanding of what was going on. To summarize what I had found:
- The foreskin (or prepuce) is a man’s most sensitive erogenous zone, more well-developed in humans than in other species of mammal. It has unique sexual functions (more on that later), which circumcision effectively destroys — and this is intentional:
- Although foreskin-chopping was once a purely religious or cultural practice, it was introduced to American medicine in the late 1800s, as a ‘cure-all’, thanks to the trend of pathologizing (treating as illness) normal human sexuality and healthy genitalia.
At the time, many doctors believed that sexual stimulation and ejaculation literally drained men of their vitality and caused all manner of illnesses and mental problems. Semen was thought to take a lot of blood to make, and losing one ounce was considered the equivalent of losing a quart of blood. Painfully severing the man or boy’s most erogenous zone was recommended, and in orphanages, it was more common to sever the penile nerve as well. This was meant to traumatize and discourage him from masturbating, lest his health deteriorate from excessive ejaculations (which was diagnosed as “spermatorrhea”).
Yes, really.
There were many quack remedies in the 1800s to improve men’s virility and erections, and to keep them from losing semen via masturbating and nocturnal emissions. This was not considered a contradiction because a man’s purpose was thought to be saving his sperm for making babies.
This may be a shock to some, although my readers may be more familiar with the ancient belief that women suffered from a vague illness called “hysteria”, especially if they experienced such “symptoms” as sexual desire and vaginal lubrication. Typically, this was a “disorder” of women who didn’t have husbands, or whose husbands left them wanting in bed, and it was thought that the buildup of sexual fluids such as “female sperm” (ejaculate) were poisoning them. In order to relieve “hysteria” symptoms, the two-thousand year old wisdom of treating it involved “massage” techniques of the “womb” (vulva), in order to induce a “hysterical paroxysm” (orgasm).
For doctors in the 1800s, this was hard work, so often they recommended a midwife to do this, and later on invented a number of vibrators and water jets that were much more effective. The fact that vibrators were the fifth household appliance to become electrified is a testament to the pathologization of women’s sexuality, not to their sexual freedom, as is popularly imagined. (That part happened later.)
Importantly, this treatment was not openly considered to be sexual because it did not involve penetration, thanks to the male-centered view of sex. This is how masturbation (that is, without a medically-sanctioned device) could be thought of as causing illness in females. However, there was another, less popular “treatment” to discourage “irritation” and “over-stimulation” in females — excision of the external clitoris. In other words, medicalized ‘female circumcision’. Various forms of this practice appeared sporadically until the 1970s, and were even funded by Medicaid and promoted for the same reasons as male circumcision (appearance, cleanliness, health, etc).
It may come as a shock to find that in the U.S., many widespread popular beliefs about the penis today are actually based on the same Victorian Era quackery rather than medical science. Indeed, the non-therapeutic circumcision of infant boys has continued to be medicalized in the U.S., and to a lesser extent in Canada, due to such persistent beliefs. Thanks to Lewis Sayre, notable surgeon and pro-circumcision quack of the 1870’s, one example is the pathologization of completely normal infant foreskins.
This continues today in hospitals, thanks to continued ignorance about penile gross anatomy: attempts to ‘fix’ the child’s normal foreskin often result in severe injury and pain. More about this shortly.
Non-therapeutic circumcision of boys by medical professionals did spread to a few other countries — most of which have long rejected it on the grounds that it is extremely harmful, with no significant medical benefit. As for the few cultures that continue to give routine infant penis-reductions a veil of medical validation, the justifications for it depend on the culture and era. In other words, it is based on local beliefs, not science. The scientific literature reveals the physical, neurological, and psychological harms of this tradition, but these are creatively ignored or glossed-over in much of the U.S. medical community.

This past April 28th, the Seattle Atheists invited John Geisheker to correct some of these myths. He is Executive Director and General Counsel for Doctors Opposing Circumcision (DOC), an organization which opposes the unnecessary genital surgery of any child.
His presentation was video-recorded and uploaded on YouTube, so if you’re interested, you can watch the video below before continuing.
Circumcision: At the intersection of Religion, Medicine, and Human Rights
I have handily rehashed most of what he says in the rest of my article, partly thanks to the notes I took — which you can see me doing in the center of the frame.
So, how did an anti-sexuality practice of the Victorian Era ever become normalized and progressive? And, what was missing from all those anatomy books, anyway? Even anatomy books I’ve seen that include the foreskin do not have a detailed visual representation of it, nor do they have much description beyond saying that’s skin that covers the tip of the penis. But it isn’t.
An anatomy lesson that a medical professional should not need:
The male prepuce, or foreskin, is a highly mobile and extraordinarily sensitive double fold of tissue that is the end of the penis. During an erection, it rolls back and inside-out, unfolding until it covers much of the penile shaft. The rest of the time, its specialized mechanisms cause it to spring back into place over the delicate mucus membrane of the glans (head), where it serves a protective function, much like your eyelids. Even in this position, it can easily be retracted simply by pulling the skin of the shaft toward the body:

While Europeans, Chinese, Japanese, and most other people may wonder why anyone would need to explain this most mundane fact, the truth is that the foreskin is not well-understood in U.S. culture and medicine. One of Geisheker’s jobs is tracking cases of American doctors who are so outrageously ignorant of intact penile anatomy that they cause serious pain and injury, usually to infants.
They don’t even know the following basic facts, so read carefully:
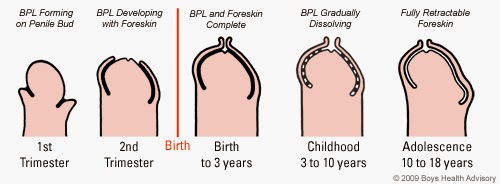
- At birth, a boy’s foreskin is fused to his glans via a membrane called the balano-preputial lamina (BPL). Much like the membrane that fuses the fingernail to the finger, it acts as a living ‘glue’.
- The same is true of the prepuce and glans of the clitoris: The female foreskin is also called the ‘clitoral hood’.
- Over the years, little ‘pearls’ of the membrane die off, thus gradually separating the foreskin and glans, creating the preputial space. (This is also true of the clitoris.)
Important to this process is a compilation of sebum and other protective secretions that mix with these dead cells, thus creating the same stuff that coats the squishy bits of females. This anti-bacterial, anti-viral and anti-fungal substance works its way toward the tip of the penis so that these ‘pearls’ can be ejected. It is still known by the Latin word for ‘soap’ — smegma.
In U.S. popular culture, smegma is contradictorily regarded as completely benign in females, yet as a volatile disease agent of the male foreskin. (More accurately, I should say, it is not recognized as smegma in females.) By around 10 to 15 years of age, the boy is able to fully retract his foreskin. This is an everyday fact in most people’s experience, except in cultures where infant circumcision is so common that doctors exist who have lost almost all knowledge of the foreskin.
Such is the case in the U.S., where there really are doctors who think an infant’s healthy foreskin is abnormally tight. Thus, they may forcibly retract it, tearing the membrane and causing lots of bleeding, excruciating pain, and further problems — much as tearing off a fingernail would. This injury can leave scar tissue, causing the foreskin to actually become abnormally tight. Such problems, as well as its natural non-retractibility, can be enough for the doctor to decide this part must be be defective and needs to be removed.
Another supposed abnormality of the infant foreskin is the free-moving tip, which can extend well beyond the glans. It contains muscle fibers which allow it to close itself like a drawstring over the urethra (urinary opening). These fibers relax when the baby urinates, keeping the foreskin wide open and pulled back, away from the urethra. At other times, they draw the end of the foreskin together to prevent contaminants (such as what may be found in his diaper) from getting inside. This normal contraction of the foreskin’s muscle gives it a long and narrow appearance and can be misinterpreted as being “too tight” or “redundant”. Smegma also creates an oily, waxy barrier which protects the infant’s glans from the irritation of urine. Without these layers shielding the urethra from E. coli and other nasties, the infant is more predisposed to urinary tract infections.
Buildup of smegma is completely harmless, yet it has been demonized in the anti-masturbation craze as causing illness. Thus, frequent cleaning of smegma is recommended by doctors who still believe the B.S. — yet, the foreskin gets in the way. Both the normal fusion and muscular contraction of the infant foreskin is considered a disorder in American medical literature, called ‘phimosis’. This false diagnosis must be corrected repeatedly in the literature by doctors from abroad, as well as such organizations as DOC.
Premature forced retraction, a colossal failure of some medical professionals (an estimated 100,000 cases in the U.S. per year), is what Geishsheker calls ‘the gateway drug’ to circumcision. Near the end of his presentation, he also reads a recent and heartbreaking letter he received from a woman whose pediatrician did this to her son, without even asking her first. The boy was traumatized by this, screamed in pain every time he urinated or was washed, and woke up screaming for five nights in a row. On top of this, she was billed $100 for ‘penile surgery’.
The foreskin has long been ignored in American medical training, and according to Geisheker’s sources, 67% of medical books do not depict a foreskin at all. Not surprisingly, that seems to be consistent with my own observations of various medical and anatomy books over the years.
In 2005, Avery’s Neonatology said that circumcision is so common in the U.S. that observations of the foreskin must be made in countries where it is not usually practiced. Even so, the U.S. medical community isn’t paying enough attention to these observations.
A survey taken at a 2009 meeting of the American Academy of Family Practice found that only 3 of 113 participants understood how to care for an intact penis. (Of course, this also suggests they didn’t have their own point of reference.) An American Academy of Pediatrics survey in 1981 showed that 78% of pediatricians gave obsolete or dangerous advice concerning an intact penis. This organization consists of both pro- and anti-circumcision doctors, and that wasn’t the last time it issued bad advice:
- In 2012, the AAP’s recommendation for cleaning babies’ foreskins is to retract them — thus tearing the foreskin and glans apart — and to wash the bleeding wound with soap and water.
- The soap, of course, causes inflammation and can lead to infections and other serious problems. Yes, this is an erroneous example of “medical advice” for infants in the U.S., although in most of the world, the advice is, basically, “leave it alone, it takes care of itself.”
- In fact, a male should not use soap beneath his foreskin for the same reason that a female should not wash her own internal bits with it: It changes the pH of those areas and causes inflammation, which can lead to imbalances of microflora and infection.
The AAP also said that “adhesions” (the natural fused condition of the foreskin) will “resolve” by 2 to 4 months of age. As I’ve mentioned, the foreskin doesn’t fully retract until around puberty, when the boy is most ready to use it.
“I just find this astonishing,” says Geisheker, of the fact that there are still medical professionals who don’t understand this ordinary, basic bit of anatomy.
So, how did all this ignorance start, anyway?
Circumcision, as I mentioned, has been a tradition of some religions and cultures going back thousands of years, including the priests of Ancient Egypt. Geisheker explains a bit of the history centered around the Jewish blood sacrifice of penile bits, and how it changed in Ancient Greece from removing the tip of foreskin to removing the whole thing. During the middle ages, Jews were discriminated against for this practice, which includes the mohel (ritual circumciser) sucking blood out of the wound with his mouth. Anti-semitic Christians invented superstitions about how this was how Jews drained babies of blood and ate their flesh. However, none of this explains the complete lack of foreskins from so much of the U.S. culture and population — which is only 2% Jewish.
This modern-day phenomenon has its roots in the 1800’s, when sexual pleasure was considered immoral. It was also when doctors had all sorts of strange beliefs about ‘vital energy’, and weren’t quite sure what caused diseases. You know, the good ol’ days, when homeopathy was a better bet than some of the treatments of medical doctors. One outmoded belief was that people start with a certain amount of energy and inevitably run out. A pre-scientific model of disease based on this idea was called ‘Reflex Neurosis’, which pathologized genital stimulation. It literally meant ‘self-nerve overstimulation’: If you touched your highly-innervated genitalia (whether sexually or not), you would drain yourself of energy, and a disease would occur in your lungs, eyes, heart, etc. It was also believed that men would eventually run out of sperm, and that ejaculation was injurious to the health — and moral constitution! Many people not only shunned masturbation, but were terrified of losing “life force” through nocturnal emissions.
In order to prevent boys from having emissions, as well as erections that are part of a normal sleep cycle, some parents were conned into buying all manner of horrific devices designed to associate pain with the genitalia. There were penis-cooling devices, contraptions with spikes on the inside, and even one that activated a phonograph player. Chastity belts were a product of this era, rather than medieval times, as is commonly believed. They were invented, along with armored night-wear, to sell to parents as a way to keep their kids from causing themselves “harm.”
In Battle Creek Michigan, anti-masturbation big shots such as surgeon John Harvey Kellogg, recommended punishing both girls and boys for “self-abuse” by holding them down, kicking and screaming, and excising their most “abuse”-prone parts. The trauma of genital mutilation, as well as the resulting loss of sensitivity, were meant to keep these adolescents from wanting to do it again, lest they make themselves sick. (This is clearly stated in Kellogg’s Treatment of Self Abuse and its Effects). A bland vegetarian diet was believed by many to curb sexual feelings, and so Kellogg also invented Corn Flakes, and provided them at his sanitorium in Battle Creek Michigan — along with yogurt enemas and electrifying baths. (Yes, very much like in The Road to Wellville.)
Kellogg believed that all sex was harmful, claimed to have never had sex himself, and adopted 42 foster children — who I don’t envy. He would travel around the country, paying various medical societies to have a Chair of Circumcision for promoting genital mutilation as a health measure. In girls, he preferred using carbolic acid to burn off the external clitoris. (Later forms of medicalized ‘female circumcision’ were not usually as extensively harmful, or even done for the same reasons.)
When this was being promoted in the U.S. and some other countries, even the female circumcision rituals of foreign cultures were interpreted as being done to get rid of ‘foul-smelling’ smegma in females, thus ignoring their religious significance. This eventually came to an end in the twentieth century, partly because it was so widely believed that women had no sexual needs unless they were mentally deranged. The fact that we know sexual stimulation is healthy is a great reason to stop circumcising both girls and boys.
A Unique Erogenous Zone
Although the technical details are known today, the foreskin was already well-understood by Renaissance anatomists as to be the most erogenous part of the penis, while the glans was known to be the dullest. This knowledge carried on into the 1800s, which is why the Americans (and later, other Anglophones) targeted it in their anti-masturbation crusade. Let’s take a look at its role in sexual function, as understood by modern medical science:
The Semmes-Weinstein esthiometer is used to test skin sensitivity for patients with burns or neuropathy. The readings from a man’s foreskin, particularly the mucus membrane of the ‘lip’ and inner surface, go off the high end of the scale.
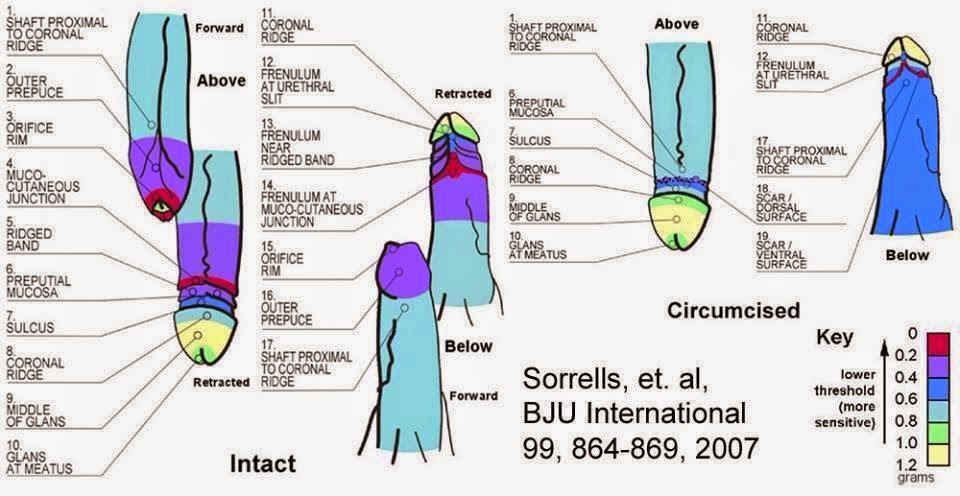
A 2007 study, published in BJU international, mapped the fine-touch sensitivity regions on circumcised versus intact penises, concluding that:
“The glans of the circumcised penis is less sensitive to fine touch than the glans of the uncircumcised penis. The transitional region from the external to the internal prepuce is the most sensitive region of the uncircumcised penis and more sensitive than the most sensitive region of the circumcised penis. Circumcision ablates the most sensitive parts of the penis.” (Emphasis mine.)
The authors’ fine-touch maps can be seen below, but first a bit of explanation about what is pictured in their illustration.
The foreskin is packed with fine-touch nerve endings called Meissner’s corpuscles. You can sort coins by feeling the edges using the front of your hands, which are dense with Meissner’s corpuscles, whereas this is not true for the backs of your hands. In the U.S., the glans is popularly imagined to be the most sensitive part of the penis, but in fact it is dominated by free nerve endings, which primarily sense pain. It has about the same fine-touch sensitivity as your earlobe, and wouldn’t be of much use for penile coin-sorting (if you’re into that). The glans is less of an erogenous zone and more of a device to hold the foreskin in its proper shape and to keep the inner surface moist: Its presence only makes functional sense when one considers it is meant to work with the foreskin.
Since most people of the world know this next part, I feel as though I’m trying to reach folks of some remote, uneducated village when I explain this:
- As the penis becomes erect, the foreskin is pulled back, rolling inside-out, everting its most sensitive areas, and (usually) exposing the glans. It can also be retracted simply by pulling the skin of the shaft toward the body. (You can view an animation and videos here.)
- When fully retracted, the foreskin is just about sufficient to cover the entire shaft: Although the length varies, it makes up approximately one half of the skin on the penis.
- What is removed by circumcision is about three inches long and five inches in circumference — think of a 3×5 index card. That’s the actual size. Although it is sometimes described as a ‘tiny little piece of skin’, this is only true of tiny little infants, not sexually active men.
It seems almost a joke to think that so many adults in such developed Western regions as the entirety of North America are completely unaware of this. Sadly, it’s not. I was once inspired to show a few such people two pictures of the same intact member — one hanging and one standing tall — and most of them thought that the erect one was missing its foreskin. They didn’t realize that it retracts! This relates to misconceptions I’ve heard that the glans is most sensitive, that the foreskin impedes sexual function by covering the glans during intercourse, and even that circumcised men have more sensation and a richer sex life because of this. This is maddeningly contrary to the facts, as we shall see, with a detailed understanding of what this sexual structure is and does.
The human foreskin contains up to 20,000 nerve endings, which is significant, since they make up about half the nerve endings of the entire penis. In fact, the human penis has a more innervated and well-developed foreskin when compared to other mammals — including our close cousins, the sex-crazed bonobos. So, we must ask ourselves, why would millions of years of natural — and sexual — selection, result in humans having an unusually large and highly-developed foreskin (and a larger glans to work with it), if it were somehow harmful, disadvantageous, or “vestigial” as is popularly believed?
True to its retractile nature, the foreskin is made to be pushed back and inside-out as it slides into the vagina, so that its more sensitive inner surface is exposed to the vaginal wall. As the penis is withdrawn, the foreskin is pulled forward again, so that it squeezes against the sensitive ridge at the base of the glans, and perhaps farther. This inside-out motion, partly aided by the foreskins’ own muscular action, is unique in human physiology: It allows the man to roll the skin of his penis against itself, either during sex or just by grasping his shaft with two fingers and thumb. This creates a gliding sensation that is not abrasive or drying to the partner. Indeed, the foreskin adds its own lubrication and erotic scent from smegma, which is laced with pheromones. This scent is revealed only when the man gets an erection, so it’s not as though he always smells, as my friend Bill had imagined. It is important in chemical signaling for the female, just as female smegma is an important signal for the male. In most cultures, the smell of smegma is widely considered a turn-on in both females and males. It is unclear exactly how important this is to human sexuality, but it is interesting to note that circumcised male lab rats have trouble finding a mate.
Without the foreskin’s action and natural lubrication, the glans may tend to ‘squeegee’ away the vagina’s own fluids, often requiring the repeated addition of artificial lubricant (this is no joke: it’s a real problem for me). Another common complaint is that the non-moving skin of the circumcised penis (even with a condom) creates friction and even microtears in the vagina or anus of the partner. This, as you may guess, can precipitate the transmission of HIV and STDs in general (also, the pain stays with me for days). However, the movement of the foreskin (with or without a condom) prevents any friction at all. This is generally preferred by sexual partners who have had experience with both, although the percentage varies somewhat by culture.
At least since the Taylor study in 1996, the specialized structures of the foreskin have been known — although I have yet to see an anatomy book that mentions them at all. Two are rather important for this discussion:
- The most erogenous tissue of the foreskin is to be found in the frenulum and ridged band. A frenulum is a cord-like fusion of flesh which holds a moving structure to a fixed structure, like the one found under your tongue.
- The penile frenulum anchors the foreskin to the underside of the glans and is highly sensitive to stretching (which it does a lot of during intercourse and masturbation). It is partly or totally removed with circumcision.
Contiguous with the frenulum is the ridged band, a ring of ridges just inside the tip of the foreskin. Each ridge has three times the density of Meissner’s corpuscles as your fingers. When the member is flaccid, this band serves a protective function in sensing foreign objects around the urethra: The sensitive ridges in your lips and anus partly serve a similar function in guarding those orifices. While engaged in vaginal intercourse, the ridged band is rolled far back on the penile shaft, facing outwards. This may have evolved to encourage deeper penetration, thus getting the sperm closer to the eggs. Much like condoms with large ‘ribs’, the outwardly-projecting ridges stimulate the sexual partner. The ridged band also ‘catches’ on the clitoris and inner labia of the female, suggesting that these structures co-evolved for this purpose. On the out-stroke, the ridged band is pressed between the partner and the coronal ridge of the glans. The ridged band is usually removed entirely by circumcision.
You can see the ridged band and frenulum in red here, which indicates the highest sensitivity level (or lowest pressure needed for the subject to notice it) as measured using Semmes-Weinstein monofilaments. The yellow of the glans indicates the least sensitive tissue, requiring 1.1 grams of pressure.
I have also learned of many pleasurable acts that can be done with a foreskin that circumcised males cannot do. For example, a partner can pull the foreskin forward over the glans and slip his/her tongue between them, thus stimulating two surfaces at once. Another technique involves pulling the foreskin forward and outward and directing a jet of water to flow underneath it. Even just pinching the foreskin shut during urination, allowing it to ‘balloon’, activates its stretch sensors in an unusual way (this also can happen naturally when a boy’s foreskin is partially separated, which is harmless, but sometimes confounds parents). Such inflation can also be achieved with air — a different type of “blow job”, shall we say? It is also possible to use the muscular tip to stimulate the nipples, clitoris, or other parts of the partner. In the case of male-on-male sex, there is the practice of ‘docking’, which means to pull the foreskin forward so that it envelops the partner’s glans. If both partners are intact, they can do ‘double-docking’, with one foreskin within the other. In fact, stimulating only the most erogenous areas are enough to elicit an orgasm. Indeed, the foreskin is thought to play an important role in controlling and modulating male orgasm.
Geisheker challenges the audience to find a book in the University of Washington medical library that says the foreskin is the seat of sexual sensation. Most medical books do, but all the books at UW he has seen have incorrectly said it is the glans.
This is also what Bill had told me, back in 2002, after revealing his shocking news. (But who could blame him? He got that from a medical text!) He also said that the foreskin was the least sensitive part of the penis, which is also a common belief I have heard. He insisted that the part’s only function was to protect the glans, and is no longer needed because humans wear clothes. What I discovered at the library was that the glans is covered in mucus membrane and is meant to be an internal structure which can be exposed, like the tongue. When left exposed to the outside world for weeks, the glans develops a layer of dead, dry skin — especially when there is clothing rubbing against it — thus blocking the sensitivity of the underlying nerves. If the foreskin is restored and the glans is re-internalized, this callus will actually dissolve within two weeks, improving sensitivity. (BTW, this can be done via ‘tugging’ devices or even tape, which expand the tissue without surgery. Such techniques are becoming popular as awareness of these facts spreads).
Bill had been right in saying that the foreskin has a protective function, but he was wrong about the details: One aspect of this function involves the dartos fascia, the layer of muscle fibers that pulls the scrotum towards the body. As I have hinted at already, this layer is also found in the foreskin, which allows it to close over the glans and pull it inward. This is handy in cold water, and even helps to prevent frostbite. The smegma of the inner surfaces also contains chemicals and immune cells which protect the penis from microorganisms and viruses. For more information (and citations) on foreskin functions, you may want to start here.
To say that circumcision has no effect on sexual pleasure or function is to be dishonest about how the penis works, or neurology, for that matter. Indeed, removing such an extensive amount of penile nerve feedback can cause a number of problems, from erectile dysfunction to premature ejaculation, which are more common among circumcised men, and which can develop in men after circumcision. Other problems include tingling, numbness, a significant decrease in sexual sensation, and even debilitatingly painful over-sensitivity. Results vary because the cause involves destroying and damaging complex, densely-innervated structures, the remainder of which must then heal and re-wire themselves to the brain in one fashion or another.
Although the literature shows that men who are circumcised work harder for sexual satisfaction, and to this end must practice more types of stimulation, this is re-interpreted by pro-circumcision advocates to mean that circumcised men have more fun and get more oral sex.
At TAM 2012, I talked to a man from Denmark, who told me that some girls get the idea from American porn that vigorous motion and lots of lubricant is needed to stimulate a man. As they become more experienced with Danish men, who are almost all intact, they find this not to be the case. I actually wrote about this encounter near the bottom of this post. Indeed, there are a few studies that purport to show that circumcision has no effect on penile sensitivity or sexual function. That is because of fatal design flaws, including that the scientists are measuring everything but the foreskin.
What they found was that the sensitivity of the glans and shaft skin are not that much different whether or not you have a foreskin, yet they are completely silent about the sensation that comes from the foreskin itself. So, nearly half the penis’ sensitivity is entirely omitted and ignored, rendering this research worthless. To conclude that removing the foreskin doesn’t affect the penis is to pretend that the foreskin is not part of the penis. This page gives a pretty good analysis of these studies in detail, as well as the effect on sexual partners, and comparing infant versus adult circumcision on sexual function.
As for the idea that the foreskin is not part of the penis, this is actually a deeply-rooted cultural belief. I remember this occurring to me in 2006 when riding in the backseat of a friend’s car one rainy night. The rear windows were fogged, and the person next to me made a mark by touching the glass, saying “I think I’ll draw a penis.” Because it is difficult to draw anything in a moving vehicle, the drawing turned out a bit misshapen, so he said, “Well, it can be an uncirumcised penis.” Something clicked in my mind. To him, a penis was always circumcised, unless it had a foreskin “added” to it.
Wait… what?
That would explain why I had heard the foreskin described as “extra” skin. If it’s normal (standard equipment), how is it extra? This parallel reality was no doubt created as a way to make this operation more palatable to people who don’t want to believe they or their loved ones were harmed by it.
Some have said that I’m against letting a man have the freedom to harm himself in this way if he wants, but this is not so: I would, however, insist that he understand the consequences, as he will have to live with them. Many adult men who chose circumcision for themselves have regretted it, and some who have chosen it as medical treatment were misled into thinking that it was the only or best treatment option when it was not. For example, a genuinely tight foreskin can often be fixed with stretching, steroid cream, different masturbation techniques, or even surgery which does not remove tissue. Some guys, unfortunately, did not educate themselves and were misled into thinking that foreskin removal was their only hope.
In 2005, I interviewed a guy who had at age two, bizarrely, retracted his own foreskin. The injury this caused to his frenulum led to pain and bleeding during sex, and his doctor told him that it needed to be removed, along with the rest of the foreskin. He went along with the operation, if reluctantly. After the intense pain had subsided, he found that he had lost a lot of sensation, responsiveness, intimacy, and confidence. He had to learn how to achieve orgasm all over again. He had traded a medical condition for an overall decrease in sexual satisfaction. He felt a very strong sense of loss and grief for two years before he was able to pull himself back together and adapt, which you can read about on my ancient blog post here. It’s just one anecdote among many, but along with the scientific data, it shows that there can be a real difference.
In European, Japanese, and other cultures in which circumcision is very rare, they have developed a substitute surgery called a ‘sleeve reduction’, or removal of a section of penile skin from the shaft. This permanently retracts the foreskin and gives the look of circumcision, while exposing the most erogenous tissue on the outside. Although this is still damaging and painful, it shows that the people of some cultures value the foreskin too much to cut it off.
When a man voluntarily has his own genital bits cut off, it is his choice, based on the information that he knows. But how can we justify his doing it to another human being who has no idea of what is going on and cannot defend himself?
I am talking about the infant, usually screaming in pain, or the young boy who only knows what others tell him about what is being done to him. Most intact men would not choose this for themselves. Although circumcised boys are usually told what was done to them and that it was for the best, some reach adulthood before they learn what was done to them. If this was so shocking for me to learn, imagine how shocked they must be at the ignorance of their own bodies!
Because Bill was a hardcore believer in the myths his parents taught him, he was so stunned at the information I found that he refused to believe any of it for some time. I brought him photocopies and printouts of journal articles and medical texts, but he rolled his eyes at them.
“The foreskin can’t have any real function,” he said, “otherwise they wouldn’t cut it off.” (“Appeal to Consequences“, anyone?)
Fraudulent Diagnoses, False Benefits, and Questionable Ethics
As we know, the reason it is cut off is because it has a very definite function, which was most threatening to many Americans of the Victorian era. Even more, a tight foreskin was thought to cause all manner of illness, from hydrocephalus to lunacy. In his presentation, Geisheker brings up the 1881 assassination of James A Garfield by the insane lawyer, Charles Guiteau. Famously, Guiteau danced to the gallows, recited a poem, and shook hands with his executioner before hanging. Upon autopsy, it was discovered that his foreskin was tight, and so his insanity was blamed on that. Such was the mentality of the people at the time.
This ‘diagnosis’ can largely be blamed on a medical doctor named Lewis Sayre, who claimed to have cured a boy of Polio by circumcising him. Like many others of his ilk, he had no proof of this, he just assumed so because the patient never returned.
I wouldn’t have, either.
In 1870, Sayre gave a speech about the harms of normal foreskins, which he called ‘congenital phimosis’ (cannot be retracted) and ‘Adhered Prepuce’ — in other words, the normal fusion found in boys until at least ten years of age.
Today, there are still some doctors who apparently think that a normal, healthy foreskin is ‘adhered’ in ‘congenital phimosis’, or even ‘redundant’ for its long, tapered look. In the billing book for medical procedures, a Code 605 refers to “redundant prepuce and phimosis, adherent prepuce, phimosis congenital.” Many healthy children are fraudulently diagnosed and subsequently circumcised under this billing code — because there is nothing wrong! Wait, what?
The process of circumcising infants has been brutal, especially since it was once assumed (also thanks to 1870’s pseudoscience) that infants do not feel pain. That’s right — even open-heart surgery has been performed on infants with zero pain control.
In reality, the younger a child is, the more pain he or she experiences, and it is especially acute in newborns. These facts, and their relation to infant surgery, did not begin to be explored until the 1980’s.
In 1934, the Gomco clamp was invented to minimize the likelihood that the infant would bleed to death if someone other than a surgeon did the operation, and without any type of pain control. The erogenous tissue is torn from the infant’s glans and crushed, excruciatingly, into goo. When the clamp is removed ten minutes later, the wound doesn’t bleed. The shallow bell is actually meant to maximize the amount of erogenous tissue that is lost. And yes, it is commonly used today in U.S. hospitals, with little pain relief, if any: this is because anesthetics are dangerous and not fully effective in infants, including nerve block techniques.
Another circumcision device is the Plastibell clamp, which strangles the erogenous tissue over an entire week. The pain and discomfort from this process commonly interferes with breastfeeding, sleep cycles, and parental bonding. Whatever the method used, the glans is afterward revealed as a raw, open sore, and the infant is almost never prescribed pain relievers. When he urinates, the ammonia burns the open sore. This wound takes weeks to heal, and complications (besides the intended damage) are not as uncommon as is widely believed. Meatal stenosis isn’t counted as a ‘complication’ because it doesn’t occur until three months after the procedure, and sexual problems of course do not count because they become evident much later on. And there are more problems which are not mentioned.
Ironically, the study of anesthetics on infants during circumcision has had to stop because it is considered to be grossly unethical. The intense pain (measured in infants’ stress responses) is far too high to justify further study.
Typical pain responses include an extremely fast heart rate, very high levels of cortisol (stress hormone), and high-pitched screaming, sometimes until the infant turns blue from lack of oxygen. The fragile newborn’s heart, lungs, and other organs can be damaged or ruptured from being overworked. Although some parents may believe that their own son “slept through” his circumcision, this is what they are told when their baby goes into shock and doesn’t respond to any stimulus. These are exactly the type of responses that we would expect in an adult whose genitals are being torn apart, yet this may be framed as ‘discomfort’. Wouldn’t ‘torture’ be more appropriate?
This extreme trauma is known to cause a sort of PTSD in infants, similar to the effects of other types of surgery or a traumatic birth, and can lead to a variety of psychological and emotional problems later on in life. It doesn’t matter whether the individual has any conscious (“explicit”) memory of this because most types of memory are stored outside of conscious awareness in the involuntary (“implicit”) systems of the brain and body. Similarly, circumcised infants, as with preemies given a heel stick or scalp IV, show neurological changes that cause a permanent increase in sensitivity to pain. In other words, intense pain in an infant re-wires the brain for life. I should also note that compared to intact boys, the circumcised ones tend to be more irritable, have trouble eating, sleeping and thriving, and demonstrate a significant increase in ‘colic’ (crying for no apparent reason) for up to a year after this ‘procedure’. A whole spectrum of emotional reactions to being put through this in one’s infancy become evident later on, and they (naturally) include a sense of loss and grief. Although foreskin reconstruction is becoming more popular today, with its own market, it was only in 1990 that desiring one’s lost foreskin was suggested to be a form of “body dysmorphia”.
For more information, and citations, you may want to start here.
As though that wasn’t bad enough, what about unintended injuries and trauma? Surgical mistakes and infections can result in more problems, from an inability to urinate, to even more tissue being excruciatingly cut away from the infant, sometimes his entire penis or more. Infections can also, more rarely, cause brain damage and death. Even if this procedure goes ‘right’, the penile skin often attempts to re-fuse itself together, resulting in abnormal adhesions, which require further tearing apart. In the long-term, the boy’s penis may grow too large to fit within the skin that is left, and may bend or even tear open when he gets an erection. This may require further surgery to add skin to his penis. Indeed, a seemingly long prepuce in infancy can turn out to be quite short in the adult. This cannot be predicted in infants, which is another good reason to wait on this question, and leave the decision to the person who is affected by it.
More popular myths that Bill told me was that the foreskin is prone to disease and is too hard to clean under to be worth the bother. In reality, the easily-retracted adult foreskin only needs to be briefly rinsed in the shower; therefore, it is easier to clean than behind one’s ears. As we shall see, this misunderstood and vilified body part has not been shown to be a vector for disease. If it was, our ancestors wouldn’t have evolved it in the first place, much less a particularly extensive one. Indeed, you don’t see other species scrubbing their penises — not even bonobos.
The cleanliness myths began in the late 1800s, with the idea of ‘moral cleanliness’ in the eye of God as he watches you masturbate. By the early twentieth century, the meme had changed to physical cleanliness and preventing STDs. However, when all the literature over the years is taken together, it shows that circumcision slightly increases one’s chances of getting certain STDs, while slightly decreasing the chances for others, and there are different statistics between cultures. All in all, it’s a wash.
Child circumcision was not common in the early 20th century, but because of the STD-prevention belief around World War I, the militaries of English-speaking countries were practically forcing sailors and soldiers to be circumcised — as most of them refused to go along with it. (In Geisheker’s audience, one guy said his uncle was an aircraft mechanic, but at 45 years old he wasn’t allowed on a Naval aircraft carrier to do work unless he was circumcised for some health and safety code. So, he was, and regretted it. Scary stuff.)
In the 1930’s, childbirth had become medicalized, and those doctors who were experts in female health (yet knew little about male health), were enthusiastic in promoting and performing circumcision on the newborn males. Their inexpertise was what the Gomco clamp was invented for.
By the start of World War II (during which we find the sand myth), newborn circumcision was beginning to become popular in the U.S., and almost as popular in Britain, although this changed when the U.K. was devastated by the war. With so few resources, U.K. doctors didn’t see any point in continuing unnecessary and dangerous surgery, so they put an end to it. At the same, the practice took off in the U.S., because it was funded by most health insurance packages, and fueled by advice from the popular press. This includes the influential child expert, Dr. Benjamin Spock, although to his credit he later recanted his position. By the end of the 1950’s, almost all newborn boys in the U.S. were subjected to this procedure, whereas almost none were in the U.K. Although child circumcision had spread to a number of English-speaking countries during the early 20th century, nowadays this practice is long-gone from most of them. And then there’s South Korea.
During the Korean War, MASH doctors imposed circumcision on the South Koreans, claiming that it improved cleanliness. Now South Korea has one of the highest penile abridgement rates in the world, and it is typically done as a rite of passage at age twelve. At the library way back when, I remember reading a very detailed report about the history and cultural beliefs about this South Korean phenomenon.
Most of the South Koreans who were surveyed believed that people from all developed countries practiced routine circumcision — which is a popular belief in the U.S. as well. These South Koreans also believed that if it wasn’t done, they had a very high chance of developing “phimosis” and needing to be circumcised anyway. So popular was this misconception that they called it “the phimosis operation”. I also recall that many adults in South Korea had this done to themselves, partly due to a combination of collectivist culture and public baths — everyone must do the same or else be looked down upon! Interestingly, those men who said that they experienced sexual problems after this operation were able to describe what was wrong, whereas those (fewer) men who said it helped their sex life did not explain how. Were they just saying what was expected of them?
And then there is the medicalized circumcision of the Philippines, which is partly influenced by Americans. Slitting the foreskin of eight-year olds (without removing tissue) has morphed into outright foreskin-severing as a rite of passage. The Filipinos have their own unique cultural myths about medicalized routine circumcision, such as that it stimulates growth in the boy, and that it will increase his virility as an adult. When you think about it, this is just as silly as the myth that a normal infant’s penis has a medical problem, that females don’t produce smegma, or that the foreskin gets in the way of sexual pleasure — and I am surrounded by people who believe these things!
Culture versus medicine
Besides cultural beliefs and customs, the only thing which supports circumcision is religious rituals. This is why the second-largest group of people to practice circumcision, after Americans, are the Muslims of the world. It is worth mentioning that most Jews in South America and parts of Europe don’t bother with this ritual anymore. As for the handful of Jews in N.Z., they fly mohels in from Australia for $5,000. And, if you’re tempted to accuse Doctors Opposing Circumcision of being anti-semitic, it should be noted that the VP is an observant Jew who has restored his foreskin.
I do think that people should be allowed to express their own religious beliefs on their own bodies, but they should not be allowed to impose their beliefs on other people’s bodies, especially children, who cannot consent or understand. The practice of withholding medical treatment from children, especially when they have cancer, diabetes, infections, etc. is widely looked down upon as severe religious abuse. So are ‘female circumcision’ rituals.
In many cultures outside of the U.S., male circumcision is viewed in the same way. Most industrialized cultures do not give routine circumcision on minors the legitimacy of medicalization. During my first library endeavors, this became clear to me when I noticed a very interesting difference between relevant entries in an American medical encyclopedia and a very similar-looking British medical encyclopedia:
- Both contained nearly the same information — basically, highlights of what I’m covering in this post — but the American version was written with a completely neutral tone whereas the British one had a distinct note of relief at the news that Americans are finally starting to learn not to chop at their infants.
- As for today, infant circumcision rates in the U.S. are continuing to drop, and are now around 50% or lower.
Even so, the Americans who have not learned have instead been inventing and recycling ideas each decade in order to justify continuing it. This includes the continuation of the old idea that it prevents sexually transmitted diseases. It is worth pointing out that New Zealand, where Geisheker is from, they stopped routine infant circumcision 40 years ago and have lower rates of STDs than the U.S.. Clearly, there are scientifically valid ways of prevention, such as sex education and condom use, which is often lacking in the U.S..
More importantly, I feel that I should point out the obvious — that infants don’t have sex. Would it not be more appropriate to wait until the individual is old enough to make a judgment about his own sex life?
The same could be said in the case of sexually transmitted HIV prevention, which is re-gaining popularity in the U.S. as an argument for circumcising infants. This connection was first proposed in a 1986 letter, by Canadian urologist Aaron Fink, who had self-published a book advocating circumcision. He promoted the unsupported claim that the callus that forms over the glans of circumcised males creates a barrier to HIV. In February 1996, Scientific American printed an article about the Caldwell retrospective analysis of HIV and its prevalence in those African populations who circumcise versus those who do not. They concluded that HIV is more prevalent among those who are intact, although they did not examine any of the patients. Vincenzi and Mertens (1994) pointed out serious flaws in the design of this study. This was pointed out in two letters to Scientific American, but they were heavily edited for publication, and the criticisms went unaddressed by the Caldwells in their rebuttal.
Even since then, most similar studies have a small sample size and contain many flaws, including guessing whether or not a subject is circumcised, based on which culture he is from. Dozens of such studies did not take into account other confounding factors such as the practice of ‘dry sex’, which creates lots of friction and tears in the vagina, nor genital ulcer disease, viral load, or female circumcision, which is only done in cultures where male circumcision is practiced. This is compounded by the fact that studies which are purported to show a connection between HIV and circumcision are more exciting, and thus more likely to be published than studies which show no correlation at all — a phenomenon called publication bias.
A 2003 Cochrane review points out all these flaws, and “found insufficient evidence to support an interventional effect of male circumcision on HIV acquisition in heterosexual men.” Also, it is worth pointing out that researchers who are white males of nations that have had a history of circumcision are the main proponents of this correlation.
The resurgence of this meme is based on three recent and incomplete studies, which were done in Africa, partly because the ethics committees in other parts of the world would not approve. Only one of these studies (Auverts, 2006) was actually published in a peer-reviewed journal. The clock for the experiment started when half of the volunteers were circumcised at random. While the intact men went off to have sex, the circumcised group had to wait four to six weeks, as they were in too much pain for intercourse. Also, they had to come back to the clinic twice more to make sure they were healing properly, where they got additional safe sex counseling and condoms. Not only were the circumcised guys unable to have sex for most of the duration of the study, but blood exposure and homosexual intercourse were not controlled for. On top of this, the researchers used an HIV antibody test, which only gives results from three months since the last exposure. However, they did not wait to administer the test, so half the cases of HIV came from before the study even started.
Based on this dubious data, the conclusion was that heterosexual men are 60% less likely to catch HIV from infected females with each exposure. And how did Auverts et al determine this? As Geisheker explains it, this study showed a very low incidence of HIV in the intact subjects, and a slightly lower incidence in circumcised subjects. It’s like comparing 1.5% versus 1%, and declaring that there’s a huge difference between the two. So, the 60% rate is relative, not absolute. If this were a vaccine, it wouldn’t be considered very effective. And the Gates Foundation is funding this.
Contrast this with condom use, which is almost 100% effective at preventing the transmission of HIV. Also, condoms protect women as well, whereas pro-circumcision researchers themselves say that circumcision only protects the man. If circumcision did protect men as they claim, the condom would still be needed. However, condoms are so effective that any small positive effect from circumcision, if real, would be superfluous. Thanks to government campaigns for always using a condom in Lesotho, Tanzania and Thailand, there are dramatic reductions in HIV. This could not and has not happened with circumcision and HIV.
There has long been plenty of evidence against the foreskin/HIV connection, even for adult men who might want to protect themselves from HIV in Africa. Even worse, some of these circumcised men believe they are protected from HIV and don’t necessarily need a condom at all. On top of that, this newest wave is inspiring some journalists and even doctors to spin fanciful tales that these African studies justify doing circumcision to infants living in quite different conditions in the U.S.. There is also some evidence in industrialized cultures that circumcision does not decrease HIV transmission, simply because the U.S. has both the highest circumcision rate and highest HIV incidence of any industrialized nation.
Another popular justification for slicing infant dicks which is trumpeted to this day is the claim that it protects against penile cancer. This idea started in the early 20th century from the circumcision-promoting Dr. Wolbarst, who proposed that smegma is carcinogenic (which was disproven), and that circumcision stops “epileptic fits” (actually orgasms) in boys. Of course cutting off a body part will prevent it from getting cancer — you can’t get cancer on what isn’t there! However, penile cancer is extremely rare, even more rare than earlobe cancer. If we think that the risk of penile cancer is worth cutting the foreskin off, then why don’t we cut off our earlobes if that is even more likely to help? Also, why don’t the folks at the American Cancer Society agree that this is a reason to circumcise infants? According to them, “it would take over 900 circumcisions to prevent one case of penile cancer in this country.” That’s a pretty extreme health measure, don’t you think?
An oncology nurse in Geisheker’s audience said that there isn’t any association at all between penile cancer and foreskins. It’s just a meme, but if you’re a lazy journalist, you’ll pad your article with these types of dubious claims and statistics. She said that when debating this issue with a urologist, she brought up breast cancer, which 1 in 12 women will eventually develop. “Would you remove breast buds off a girl?” she asked. The urologist said, “You’re right, we shouldn’t do it.” Besides, statistically, infants are more likely to die of the circumcision itself than to die of penile cancer as adults.
Indeed, infants don’t get penile cancer at all, men do, especially older ones, so again, it would make more sense to wait and let the individual judge this matter for himself.
A similar argument has been made that circumcision prevents transmission of HPV, and thus cervical cancer, in women. This is also completely untrue and based on fatally-flawed studies, which you can read more about here. What is most outrageous with this claim is the idea of causing significant and irreversible harm to an unconsenting infant, in anticipation that it may have some effect on a hypothetical female sexual partner in the future. It’s not meant to help the infant who’s being operated on, but rather, someone he may never meet. He may, for all we know, turn out to be gay. Also, such a concern of HPV should be outmoded, since there is now an effective vaccine against it.
Then, of course, there is the the tired old argument that foreskinlessness prevents urinary tract infections. This began with the Wiswell study (yes, really), which compared the rate of UTIs between circumcised with intact babies. There were a few fatal flaws, including instructing the parents of the intact boys to repeatedly retract the foreskin and wash under it. Which, as we know, is a known cause of infection — this includes UTIs.
The larger picture here, of course, is that UTIs are generally no big deal — they are easily treated with antibiotics. In fact, young girls are four times more likely to get UTIs than intact boys, and no surgery is recommended for them. There is also no evidence that circumcision prevents UTIs in adults, even though it is sometimes recommended for chronic ones. It shouldn’t be, because chronic UTIs are caused by internal problems, not external ones. In any case, it is ludicrous to put weight on foreskin-chopping in infancy as a treatment for such a minor and treatable problem, even if the literature did show a benefit. The treatment is far worse than the sickness!
Interestingly, in the United States, the highest rate of circumcision centers around Michigan, home of Kellogg — coincidence? Of course, the Midwest also has more Medicaid subsidies that pay for it. Out here in Seattle, and other U.S. locales where circumcision is not nearly as common, the children are no sicker than the ones in the Midwest.
In New Zealand, Geisheker’s home country, they completely gave up routine circumcision 40 years ago, and NZ children are healthier than U.S. children today. Also, the rate of circumcision in Australia has plummeted in recent decades, while at the same time, health among children has improved, due to better healthcare. Geisheker also works with European and Australian doctors, who think that Americans are a bit backwards when it comes to chopping babies’ perfectly healthy genitals. According to most doctors of the world, it’s a bad idea:
After reviewing the currently available evidence, the RACP believes that the frequency of diseases modifiable by circumcision, the level of protection offered by circumcision and the complication rates of circumcision do not warrant routine infant circumcision in Australia and New Zealand.
— The Royal Australasian College of Physicians, 2010.
Circumcision of newborns should not be routinely performed.
— The Canadian Paediatric Society, 1996.
There is no convincing evidence that circumcision is useful or necessary in terms of prevention or hygiene… circumcision entails the risk of medical and psychological complications… Non-therapeutic circumcision of male minors conflicts with the child’s right to autonomy and physical integrity.
— The Royal Dutch Medical Association, 2010.
While most doctors of the world discourage this practice, doctors in the U.S. frame the situation differently. Their arguments for child circumcision center around motivating parents to feel comfortable with choosing this for their unconsenting children. The parents don’t want to hear that they, or loved ones, have been harmed, and so are more willing to believe that it’s for the best.
Extraordinary claims sometimes require extraordinary justifications, and we can see some level of parallel with female genital mutilation. In one African culture that I have heard of, it is believed that when a woman gives birth and the baby’s head touches her clitoris, both will die. We know this is ridiculous, since we see that it doesn’t happen. In the same way, outsiders ridicule the “disadvantages of a foreskin” that I hear all around me, particularly if they never occur in real life.
In college, I wrote a paper on child genital mutilation (yes, really) and I remember reading an article about immigrants to the U.S. from someplace in Africa. They believed that the clitoris causes women to like sex “too much” and engage in excessive sexual behavior. When they saw a pregnant teenage girl, they would say, “See? Americans need to circumcise their daughters. I would not let my daughter keep her clitoris!” If this is shocking to you, then good: This is basically how most people of the world regard parents who say their son needs to have his most erogenous zone cut off.
Many of the immigrant women did not know what a clitoris is, nor what they were missing. This may seem dismaying to you, and it is equally so to me when I am asked by a full-grown man what a foreskin is. Even worse is the ones who don’t know, but they don’t realize they don’t know.
Only a few years ago I heard of a controversy in Egypt, where 90% of women are circumcised, over whether the female practice should be medicalized. As per Egyptian culture, some doctors recommended removing the prepuce of the clitoris, with the belief that there was medical evidence that this protects against HIV. They called this procedure ‘female circumcision’, but they called removing the entire clitoris ‘genital mutilation’. Other doctors said that was an unfair characterization and that all of this is female genital mutilation.
Since the bias against some genital parts over others is based on cultural beliefs, I wondered about other body parts that might be discriminated against. One example is to be found in a book by Carol Tavris and Elliot Aronson. The title should give you a clue — Mistakes Were Made (But Not By Me): Why We Justify Foolish Beliefs, Bad Decisions, and Hurtful Acts. It’s about how people solve their cognitive dissonance between their image of themselves as a generally good person, and facts which seem to contradict this. The book opens with the Nuer and Dinka tribes, and a much stranger coming-of-age ritual: Surgically extracting the front teeth with fishing hooks — two on the top, and up to six on the bottom.
This is extremely painful, somewhat risky, and in the long-term, causes a gradual atrophy of the jawbone, especially a caved-in chin. What could possibly possess anyone to do this to their own children? It is thought to have been their solution to an outbreak of tetanus, in order to keep children from starving to death through clenched jaws. Over the years, it became a coming-of-age rite, ‘normal’ for everyone in the tribe. Now the general opinion amongst tribe members is that people who have all their teeth look frightening like cannibals, or silly like donkeys. They also say they prefer the whistling sounds they make when they talk.
These post-hoc justifications are a way to resolve the cognitive dissonance between causing harm to children, and having had harm caused to them. Besides, it’s just normal to them! This very same point is repeatedly made by researchers concerning the U.S. bias against foreskins, and the billion-and-a-half dollar industry based on cutting them off. Indeed, there are a million routine infant circumcisions done in U.S. hospitals each year — it is among the most common surgeries in the United States.
Instead of allowing the individual to enjoy his own erogenous zone, it is tossed in the incinerator, or sold to companies such as Invitrogen for other people’s profit and benefit.
That’s right — genital parts ripped from uncomprehending infants are made into Apligraf Magic Skin Treatment, and even Oprah has been criticized for pushing a skin cream made from baby penile cells. It seems that in the U.S., the male prepuce is valued more as a commodity than as a rightful part of a person’s own body. (Yet, the reverse is true for the female prepuce.) There’s a difference between donating an organ and stealing an organ. Which is this? Whose body is it, anyway?
I once made this point to a former housemate of mine who was pregnant with a boy. Although I had previously talked with her about this subject, twice, it evidently had no effect. She personally didn’t like the look of a normal, intact penis, and wanted her boy to match his friends. I explained to her that only 30% of newborn boys are circumcised in the Seattle area, so he would actually be unlike most of his friends.
She replied, “So?”
Then I told her why most other societies in the world look down upon chopping off the most sensitive part of the penis.
She said, “Who cares what they do in other countries? I want to do what Americans do!”
I switched tactics and asked her, “Whose penis is it? Is it yours? What if your dad had part of your genitals cut off because he didn’t like the way they looked? How would that make you feel?”
Unable to answer in a rational manner, she started screaming about how it was her right as a parent to make this decision and how dare I tell her what to do, or even care about it at all, as it was none of my business.
“It’s my child, it’s my choice!” she shouted, and stormed out of the room, slamming the door. Although her emotional reaction was quite strong, it is not that different from more typical incidents I have heard of.
Indeed, instead of centering this surgery around the person who is affected by it, and letting him make this decision about his own body, I have noticed that pro-circumcision websites are all about having the parent choose. Displayed on their front pages are comments from parents along the lines of “I have never regretted my choice,” and “I agree, parents should be the ones to decide.” What about his choice? Can it wait until he is old enough to fill out a consent form? He will probably prefer to keep what he was born with, thanks. Most do.
In response to making this very point, I’ve heard, “Of course he will want to keep his foreskin, that’s why I shouldn’t leave the choice to him!” Sound familiar?
This is why most male circumcision rituals of various cultures are done on young boys — they are not large enough to fight back or leave the tribe. They also don’t usually have lawyers to protect them, although those are employed in North America. Geisheker mentions the 14 year old boy by name of Bolt, whose father had converted to Judaism and wanted his son’s penis to match his. Bolt’s case was turned down by the Supreme Court, but by then, he was old enough to testify in court. He escaped unharmed and went to live with his mom. Defending male children from circumcision is tough in the U.S. because no medical license is required — it can be done by mohels, midwives, nurses, or parents. That’s partly because it’s not medicine. In New Male Studies, Geisheker published an article about this, called The Completely Unregulated Practice of Circumcision.
Indeed, in the U.S., most doctors, midwives, and OBGYNs bring up the question, and frame it as though it is a decision to be made by the parents. Although I’ve heard of doctors in Seattle questioning parents who want to do this to their children, they could do better/ In the 1960’s, doctors in New Zealand ended the practice by not bringing it up to parents, and if anyone asked about it, they said that it was an obsolete procedure that came from England. That was usually enough to dissuade them.
American medical culture is still full of bias on this topic, as many European doctors pointed out in response to a 2012 American Academy of Pediatrics pro-circumcision technical report. Plus, out of eight people on the AAP committee, four of them had vested interests: one had circumcised his own son on his kitchen table; one was a doctor in Seattle at the children’s hospital who promoted female circumcision; one was an expert in medical financing; and one refused to reign in a mohel for giving babies herpes via sucking their penis wounds.
Near the end of his presentation, Geisheker demonstrates what Bioethics 101 means. There are a few points to consider when you focus on the patient’s immediate needs, from the point of view of the patient.
Beneficence — Is the procedure necessary/beneficial?
Nonmaleficense — Does it avoid harm/suffering
Justice — Would we choose this for ourselves?
Autonomy — Is the patient being treated as a separate person or as a member of a community? Can it wait for patient assent?
Proportionality — Is the risk and pain worth the gain?
As I hope to have demonstrated in this post, non-therapeutic child circumcision fails every one of those requirements. He comes to the same conclusion that I grasped many years ago: It is plastic surgery, a phrase that means ‘adult’.
This is so obvious to people outside of this sort of culture that they could easily assume that Americans don’t do this, just as Americans commonly assume that the rest of the industrialized world does. The first time I discussed this with a non-U.S. person, a man from Ireland, he said he had no clue of this practice until he saw a variety of American pornography. He reported feeling repulsed by the strange, vigorous way that “mutilated” genitals had to be stimulated. The people from Europe that I have talked to on this issue have all told me that in their countries, male and female circumcision are both regarded as pointless and culturally backwards.
Indeed, it is a bizarre double standard in North America and some other places that people can think that hacking at boys’ genitals is good, but that hacking at girls’ genitals is bad. I think that much of this is related to the deeply-embedded cultural attitude that the foreskin is not part of the penis. As I’ve mentioned, I’ve seen this phenomenon in person, as well as on TV and in movies. Another example is Robin Williams’ comedy routine about how wonderful the male member is, yet his only allusion to the hyper-developed erogenous zone was “an optional covering”. That is like saying that your lips are an optional covering, rather than a functional part of your mouth. I once even saw the episode of Penn & Teller: Bullshit on this topic, and laughed hysterically when the doctor actually said they use a clamp so as not to “hurt the baby’s penis”, while he screams in agony (or “tolerates extremely well”). It would be quite a feat to be able to amputate a huge section of any appendage without harming it, yet that is essentially the claim here.
“Cutting off part of the penis is not injuring it in this reality, only cutting off more than what you intended to leave,” says physical oncologist Ryan McAllister in his presentation The Elephant In The Hospital, which I’ve linked to below.
` In 2011, someone I’ll call ‘L’ posted this video on Facebook in response to his brother and wife’s adopting what was about to become most-of-a boy.
` The wife claimed that this is a religious practice required in Catholicism, which is anything but true, yet is a common belief.
` The brother, who admitted to knowing nothing at all about foreskins, said that he was satisfied in the amount of research he had done that he was making the right choice.
` Instead of clicking on the video, they simply raised a fuss, calling it a ‘family crisis’, and forbid L from ever meeting the boy.
In the hopes that someone would learn from this video, I posted it on Facebook (where else?):

Child Circumcision: an Elephant in the Hospital
Ryan McAllister, PhD What is infant circumcision? Why is the practice common in U.S. hospitals and not in other countries? What does it remove…
He brings up most of the same things that I have brought up already, and takes a closer look at some of the phallic logical fallacies of this culture:
Poisoning the well: “It’s cleaner, looks better.”
Appeal to Majority: “Everyone does it.”Minimizing words: “Little snip”, “useless”, “flap of skin.”
Special Pleading: “Babies don’t feel pain or remember.”
Appeal to Ignorance: “I can’t imagine how it could be harmful.”
He examines the cyclic view of a social surgery, that is, one that removes a healthy unique organ part. Many doctors know it’s a social surgery, not a treatment, yet they take advantage of the parents’ trust.
- They trivialize complications and don’t tell the parents that the foreskin is a sexual part. They don’t bring up ethical questions or conflicts of interest, such as profit and tissue uses.
- He actually shows a video of the surgery: The infant is screaming in extreme pain, yet the physician is not bothered by this.
- Losing one’s job is one possible punishment for doctors and nurses who don’t want to do it, or who tell parents not to.
- Not only does it harm children and their parents, it hurts the health practitioners because they are learning to harm people.
The AAP ethics committee says that it is inappropriate to allow the individual to make his own decision, and obstetricians claim that it’s the mother’s choice because she is the patient, not her child. McAllister shows a clip of an obstetrician interviewed on Craig Ferguson’s talk show. She said it really is a social and cultural procedure, and that any health benefits from circumcision can be achieved through washing.
Then she says, “You have to choose as a parent.”
“That’s a tough choice,” Craig jokes.
Do you have to choose giving your baby a nose job, too?
Because of the circumcision craze, David Gibbins, Pediatric Urologist said that in a two year period he was referred over 275 newborns and toddlers with complications from it, and almost half needed corrective surgery.
There is also the unspoken assumption that foreskin-chopping is inevitable. I have long noticed this, as in “My parents waited until I was six before they finally had me circumcised.” Also, Americans tend to use the word ‘uncircumcised’, which implies that you’re in line to do it eventually. I would not say that I am ‘uncircumcised’, or ‘unmastectomized’ for that matter. Women aren’t viewed that way, so why are men?
To my surprise, I didn’t get any dissenting comments on the video — instead, it attracted the attention of an Australian man, who I was able to relate a few of my bizarre anecdotes to, some of which I have already related in this post. I’d display those comments here, but I’m saving them for a future post.
I hope I have made thus far a fairly convincing argument that there is a clear cultural bias in this matter, based on ignorance, misinformation, and a desire to justify the damage that has been done.
Pointing out the double standard of ‘male circumcision is good’ and ‘female circumcision is bad’, has earned me accusations that I’m discriminating against females. The truth is, I want everyone to be protected from having chunks of them cut off for other people’s benefits, male, female, and otherwise. A friend of mine is a man who was born intersex, and whose penis and testicles were removed when he was an infant. His medical records were destroyed and the truth was kept hidden from him by his family and all his doctors until he finally solved the mystery himself in middle age. I know something of the anguish and impairment that social surgery can have on a person, and it goes beyond men with normal anatomy.
By the way, it’s taken me until 2015 to finally publish this draft, and this was part of what motivated me to get going: I saw one of my skepticy friends had posted a quote from a Victorian Era doctor about keeping boys from masturbating. I tried to explain how the backwardsness of this is still with us in medicine, but it didn’t work, as you can see.
If I’d completed this article by then, and thus was able to link to it, this wouldn’t have happened:
Circumcision existed long before America. It was done for religious reasons representing a covalent between God and Abraham. Here: “the procedure is most often elected for religious reasons or personal preferences,but may be indicated for both therapeutic and prophylactic reasons. It is a treatment option for pathological phimosis, refractory balanoposthitis and chronic urinary tract infection. ” And “The WHO recommends considering circumcision as part of a comprehensive HIV program in areas with high endemic rates of HIV, such as sub-Saharan Africa,”…
Nothing to do with masturbation.
I am snickering, thinking of God and Abraham sharing electrons. I will abbreviate my own responses, which threatened to become their own blog post.
First of all, the religious tradition is partly for desensitizing the penis and getting the man’s focus on heaven…. It was promoted by the co-founder of the American Medical Association and his followers….
Various myths about circumcision and medical benefits arose, which persist to this day and are not generally believed in most countries, where it is not practiced or recommended….
…It also unnecessarily maims the penis by cutting off the most sensitive part. The foreskin is as sensitive as your lips, and the glans is as sensitive as your arm. That is because it serves several purposes, including controlling orgasm. Circumcised men have the most sexual dysfunctions.
…it’s an unbearably painful thing to do to an infant’s fused penis, and can lead to long term trauma reactions. It is outlawed in many parts of the world for this and the sexual repercussions.
I could go on, but you get the idea. It is a practice to suppress sexual pleasure. It is not done in Europe, other than for religious reasons….
He responded:
Proof. Where is the proof it is an American thing? Where is the proof there is higher sexual dysfunction? Where is the proof it was/is used to deter masturbation? It is not recommended nor is advised against…
Unable to do much of an internet search, or even paste links, thanks to my malfunctioning smartphone at the time, I replied:
…Last I checked the internet and online medical journals I found pretty much the same thing.
Why not do a few keyword searches and see what you find?
…
I often talk about it with men in other parts of the world and they all think it’s nutty and wtf is wrong with Americans. One guy said he broke up with his girlfriend from South Africa because she said if they had a son she would have him circumcised because she likes having sex with circumcised cocks. This is a common attitude I have found in the U.S..
What if a man said he prefers sex with circumcised women so he does that to his daughter? Is he planning to have sex with her? Is he seeing her as a sex object?…
He didn’t respond to that well.
Proof. Where is your proof? If you are going to assert that male circumcision is an American phenomenon to deter masturbation you are making one hell of a claim. The original post had nothing to do with circumcision but about masturbation. I have seen not heard of no study that shows even correlation between circumcision and the desire or pleasure derived from masturbation
They exist. A few of them are even quoted here. I couldn’t paste any such links, however, so I replied:
It’s not based on science.
Also I did not say it’s an American phenomenon, I’m saying that the medicalization of it started in Victorian America, as part of their cultural beliefs.
In the late 1800 it became a Christian-anti masturbation medical practice….
It won’t let me paste the link, just [do a search] and the proof will magically appear, don’t tell me I didn’t give you any evidence!!
And to repeat myself, I often talk about how nutty it is with people from parts of the globe where it is not practiced as a medicalized phenomenon.
They count it as one more reason Americans are nutty.
Also in parts of Africa, some doctors are fighting to medicalize female circumcision. Does it make that legit, too?
This hardly had the effect I had hoped:
As I said in an early post, there are religions that practice it and there are medical benefits in some cases. Googling as you recommended, yes there were some who thought it would stop masturbation in addition to health reasons. About one-third of males WORLDWiDE are circumcised (http://whqlibdoc.who.int/publications/2007/9789241596169_eng.pdf)
Male circumcision is not the same as female genital mutilation.
I grow bored of this
Evidently, he was more interested in dismissing me than understanding my argument. I replied:
I didn’t say it was . I pointed that out because it is fashionable in those cultures to believe that female genital mutilation is good. [It used to be in this culture.]
You are good at putting words in my mouth.
And where do those males worldwide live? In cultures where people have traditionally done so and come up with beliefs about why they do it — mostly Muslims.
My point is, where it is done depends on the culture. Do you not see that?
Also, you should check out what Maimonides said about it, he was after all an ancient Jewish scholar. ;-)
[Maimonides says that circumcision is good because it decreases sexual pleasure for the man and the woman, so that they will keep their minds on God rather than the unclean flesh.]
At that moment, he deleted the thread, and I had thought it was because of me, although he says otherwise.
Later on, I was able to send him a link to a relevant article, one of a series. I don’t know if he ever read it.
By coincidence, Geisheker wrote two of the articles in this series, and suggests some further reading (if this post hasn’t been too much for you already):
There’s Robert Darby’s account of circumcision as a fad in Britain, A Surgical Temptation: The Demonization of the Foreskin and the Rise of Circumcision in Britain.
Also, there’s his commentary on the continued practice in America The Sorceror’s Apprentice: Why Can’t We Stop Circumcising Boys?
Also, there’s an interesting book by David Gollaher, Circumcision: A History of the World’s Most Controversial Surgery.
Anthropologist Leonard Glick wrote Marked In Your Flesh.
I also wrote up a follow-up article, which features an anatomy lesson video, biased anatomy books, a doctor saying that the foreskin is not fused at birth, crazy pro-circumcision pedophiles, doctors invented just to promote circumcision, and Facebook comments which show that indeed, it is just a cultural thing.
You can check it out at this link: Child Circumcision: Culture-based ignorance, fetish, and pseudoscience.
Read GreenMedInfo’s latest article on this topic:
Infants Deeply Traumatized By Common Medical Procedures, New Study Suggests
Originally published: 2015-04-27 Article update: 2019-05-27


'The Foreskin: Why Is It Such A Secret In North America?' has 1 comment
May 16, 2019 @ 10:54 am RadioGuGu
Cells from this tissue (the foreskin) are used in the production of (some) vaccines.